Anterior Cervical Discectomy & Fusion Surgery (ACDF)
Anterior cervical discectomy and fusion (ACDF) is a type of neck surgery to remove a damaged disc and relieve pain. A small cut is made in the front of the neck to remove the disc. Then, a graft is inserted to connect the bones above and below the disc. This surgery is considered when treatments like physical therapy or medication do not relieve neck or arm pain. Most patients go home the same day.
Healthy discs act as a flexible cushion between bones, allowing your neck to bend and rotate. Wear and tear on discs can cause herniation or thinning that pinch the nerves.
Discectomy literally means “cutting out the disc.” A discectomy can be performed anywhere along the spine from the neck (cervical) to the low back (lumbar). The surgeon reaches the damaged disc from the front (anterior) of the spine through the throat area. By moving aside the neck muscles, trachea, and esophagus, the disc and bony vertebrae are exposed. Surgery from the front of the neck is more accessible than from the back (posterior) because the disc can be reached without disturbing the spinal cord, spinal nerves, and the strong neck muscles. Depending on your particular symptoms, one disc (single-level) or more (multi-level) may be removed.
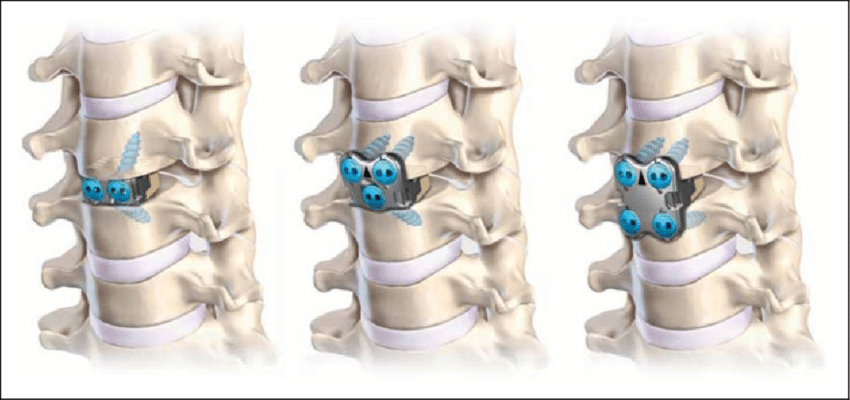
After the disc is removed, the space between the bony vertebrae is empty. To prevent the vertebrae from collapsing and rubbing together, a spacer bone graft is inserted to fill the open disc space. The graft serves as a bridge between the two vertebrae to create a spinal fusion. The bone graft and vertebrae are fixed in place with metal plates and screws. Following surgery, the body begins its natural healing process and new bone cells grow around the graft. After 3 to 6 months, the bone graft should join the two vertebrae and form one solid piece of bone. The instrumentation and fusion work together, similar to reinforced concrete.
After fusion, you may notice some range of motion loss, but this varies according to neck mobility before surgery and the number of levels fused. If only one level is fused, you may have similar or even better range of motion than before surgery. If more than two levels are fused, you may notice limits in turning your head and looking up or down.
Artificial disc replacement has emerged as an alternative to fusion. Similar to knee replacement, the artificial disc is inserted into the damaged joint space and preserves motion, whereas fusion eliminates motion. Outcomes for artificial disc compared to ACDF are similar, but it is not for those with facet joint arthritis or weak bones. Talk with your surgeon about whether ACDF or artificial disc replacement is appropriate for you.
Who is a Candidate?
You may be a candidate for discectomy if you have:
A herniated or degenerative disc
Significant weakness in your hand or arm
Arm pain that is worse than neck pain
Symptoms that have not improved with physical therapy or medication
What are the Results?
Anterior cervical discectomy is successful in relieving arm pain in 92 to 100% of patients. However, arm weakness and numbness may persist for weeks to months. Neck pain is relieved in 73 to 83% of patients. In general, people with arm pain benefit more from ACDF than those with neck pain. Aim to keep a positive attitude and diligently perform your physical therapy exercises.
Achieving a spinal fusion varies depending on the technique used and your general health (smoker). In a study that compared three techniques: ACD, ACDF, and ACDF with plates and screws, the outcomes were:
67% of people who underwent ACD (no bone graft) achieved fusion naturally. However, ACD alone results in an abnormal forward curving of the spine (kyphosis) compared with the other techniques.
93% of people who underwent ACDF with bone graft placement achieved fusion.
100% of people who underwent ACDF with bone graft placement and plates and screws achieved fusion.
What are the Risks?
No surgery is without risks. General complications of any surgery include bleeding, infection, blood clots (deep vein thrombosis), and reactions to anesthesia. If spinal fusion is done at the same time as a discectomy, there is a greater risk of complications. Specific complications related to ACDF may include:
Hoarseness and Swallowing Difficulties: In some cases, temporary hoarseness can occur. The recurrent laryngeal nerve, which controls the vocal cords, is affected during surgery. It may take several months for this nerve to recover. In rare cases (less than 1/250), hoarseness and swallowing problems may persist and need further treatment with an ear, nose, and throat specialist.
Vertebrae Failing to Fuse: There are many reasons why bones do not fuse together. Common ones include smoking, osteoporosis, obesity, and malnutrition. Smoking is by far the greatest factor that can prevent fusion. Nicotine is a toxin that inhibits bone-growing cells. If you continue to smoke after your spinal surgery, you could undermine the fusion process.
Hardware Fracture: Metal screws and plates used to stabilize the spine are called “hardware.” The hardware may move or break before the bones are completely fused. If this occurs, a second surgery may be needed to fix or replace the hardware.
Bone Graft Migration: In rare cases (1 to 2%), the bone graft can move from the correct position between the vertebrae soon after surgery. This is more likely to occur if hardware (plates and screws) is not used or if multiple vertebral levels are fused. If this occurs, a second surgery may be necessary.
Adjacent Segment Disease: Fusion of a spine segment causes extra stress and load to be transferred to the discs and bones above or below the fusion. The added wear and tear can eventually degenerate the adjacent level and cause pain.
Nerve Damage or Persistent Pain: Any spine surgery comes with the risk of damaging the nerves or spinal cord. Damage can cause numbness or even paralysis. However, the most common cause of persistent pain is nerve damage from the disc herniation itself. Some disc herniations may permanently damage a nerve making it unresponsive to surgery. Like furniture on the carpet, the compressed nerve doesn’t spring back. In these cases, spinal cord stimulation or other treatments may provide relief.
A neurosurgeon or an orthopedic surgeon can perform spine surgery. Many spine surgeons have specialized training in complex spine surgery. Ask your surgeon about their training, especially if your case is complex or you’ve had more than one spinal surgery.
What Happens Before Surgery?
In the office, you will sign consent and other forms so that the surgeon knows your medical history (allergies, medicines/vitamins, bleeding history, anesthesia reactions, previous surgeries). Discuss all medications (prescription, over-the-counter, and herbal supplements) you are taking with your healthcare provider. Presurgical tests (e.g., blood test, electrocardiogram, chest X-ray) may need to be done several days before surgery. Consult your primary care physician about stopping certain medications and ensure you are cleared for surgery.
Stop taking all non-steroidal anti-inflammatory medicines (ibuprofen, Advil, etc.) and blood thinners (Coumadin, aspirin, Plavix, etc.) 7 days before surgery.
Stop using nicotine and drinking alcohol 1 week before and 2 weeks after surgery to avoid bleeding and healing problems.
You may be asked to wash your skin with Hibiclens (CHG) or Dial soap before surgery. It kills bacteria and reduces surgical site infections. (Avoid getting CHG in eyes, ears, nose, or genital areas.)
Stop Smoking
The most important thing you can do to ensure a successful spine surgery is quit using tobacco. This includes cigarettes, vaping, cigars, pipes, chew, and snuff/dip. Nicotine prevents bone growth and decreases successful fusion. Smoking risk is serious: fusion fails in 40% of smokers compared with 8% of non-smokers. Smoking also decreases blood circulation, resulting in slower wound healing and an increased risk of infection. Talk with your doctor about ways to help you quit: nicotine replacements, medications (Chantix or Zyban), and counseling programs.